APS orders (should) plummet when you adopt Irix Medical Data
With training and management of expectations, you can avoid a possible hike at implementation time.
Medical Data often provides enough insight into an applicant’s health to allow underwriters to make a quick, cost-effective, and confident decision without ordering an APS. But many underwriters are accustomed to ordering an APS whenever a specific condition appears in a file. And since Medical Data provides significantly more insight into conditions that may be present, carriers may sometimes see an initial increase in APS orders.
Left to their own devices, underwriters will learn that Medical Data often provides sufficient insight to reach a decision without an APS. In many cases, Medical Data delivers more information than they would get from an APS due to the breadth of coverage from multiple providers. As underwriters develop trust in Medical Data, APS orders begin to drop off and eventually settle at a level even lower than before.
You can sidestep a potential jump in APS orders at adoption with training. We recommend engaging underwriters with tailored Medical Data training, where Milliman IntelliScript shares insights and best practices from a decade of Medical Data implementations.
We displaced more than 90% of APSs and are in the process of eliminating most labs ... Prescription Data + Medical Data finds most everything. — Major life insurance carrier
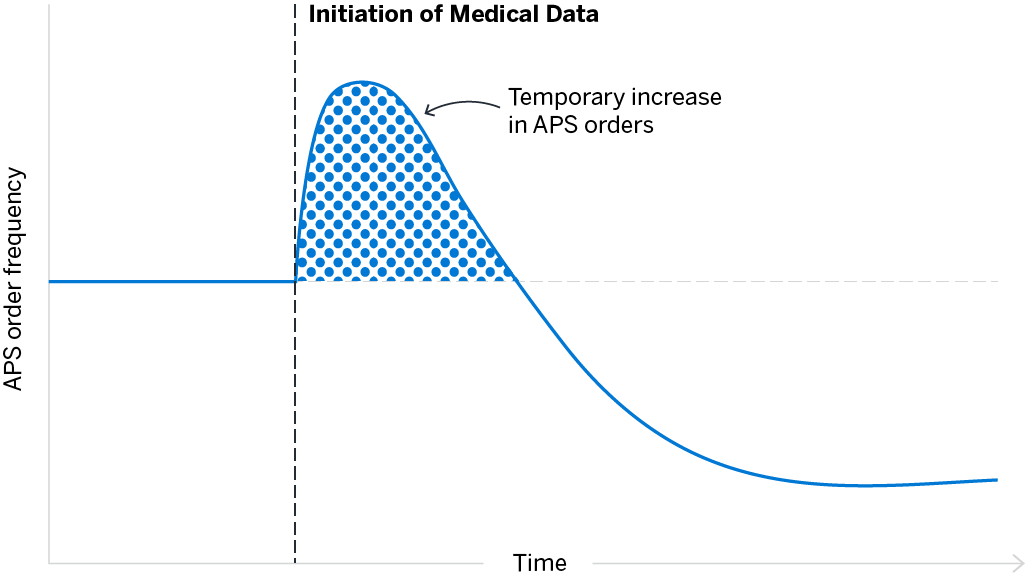
Carriers initiating Medical Data see immediate protective value and may experience a temporary increase in APS order frequency. After adjusting underwriting processes and guidelines, that temporary increase becomes a permanent reduction in APS orders.

Moving quickly to train underwriters and adjust procedures and guidelines results in a smaller increase in order frequency before orders settle to much lower level.
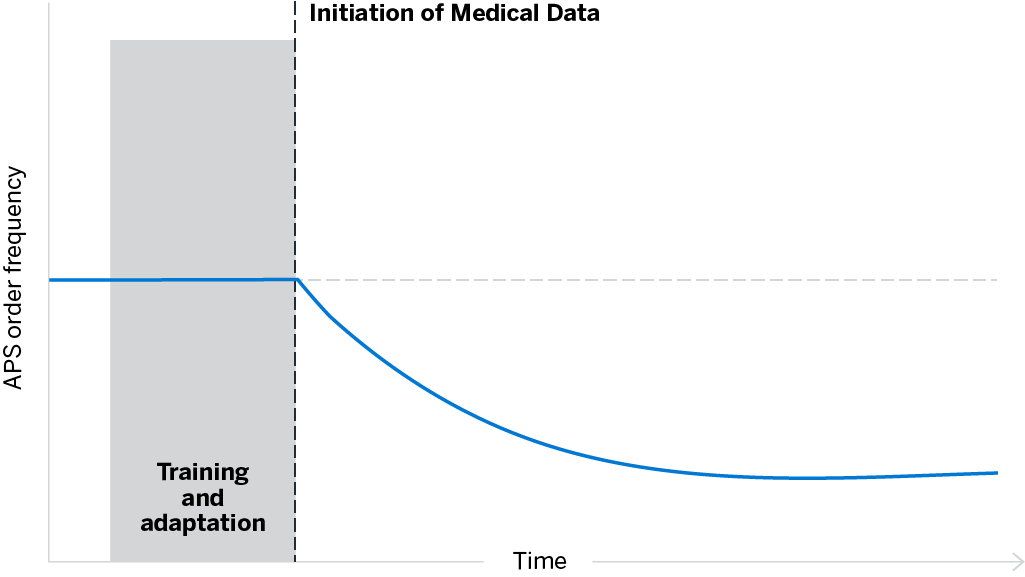
Carriers that proactively train underwriting staff and review processes before integrating Medical Data can avoid even a temporary increase in APS orders. We offer free training and love helping our customers get the maximum ROI from our products.
FAQs
Why do some carriers see an increase in APS orders after the implementation of Irix Medical Data?
- A typical Medical Data hit includes 240 codes which often present underwriters with many more potential conditions to consider than they would have seen with Rx, application, standard paramed exams and labs, etc.
- This additional data is useful and contributes to protective value, but at first it may be hard for underwriters who are seeing so much more information to trust those findings and/or focus on what matters.
- When this additional data is dropped into legacy guidelines and underwriting procedures, it may trigger an increase in APS orders.
Do carriers normally see an increase or decrease in APSs once Medical Data has become part of their underwriting process?
- Carriers that add Medical Data to the underwriting workflows find that APS orders settle to a level well below their previous usage. However as noted above, there may be an initial uptick in orders when underwriters start seeing so much more data.
What types of data are gathered for Medical Data?
Code sets:
- HCPCS
- ICD
- CPT
- REV
Encompassing:
-
- Diagnosis codes
- Procedure codes
- Durable medical equipment
- Clinic-administered drug therapies
- Places of service, including:
- Office visits
- Specialists
- Hospitalizations
- Emergency rooms
- Ambulances
- Physical or occupational therapy
- Dialysis clinics
- Home healthcare
- Hospice
Prescriber specialty can also be used to help determine whether a condition is merely suspected or has been found, as well as whether and how it is being treated.
Are all those codes treated equally by the Irix Rules Engine?
- No. The Rules Engine is set to prioritize codes that indicate conditions of underwriting concern, while parsing “noise” such as non-specific symptoms (e.g., cough), resolved diagnostic studies, etc.
- Before data gets to the Rules Engine, we remove all diagnostic codes on encounters that are strictly diagnostic in nature. These could be diagnosis codes accompanying a blood panel or even diagnosis codes entered in an ambulance ride en route to the ER. Underwriters still see the procedure codes—what was done—but working diagnosis codes are removed because we’ve found that the diagnosis codes on downstream encounters are much more useful.
- The interpretation of the resulting data has been developed over almost a decade. It continues to be refined by our clinical and actuarial staff to ensure it’s as relevant as possible.
Does Medical Data show lab results?
- We see codes for lab testing as ordered, and some codes for individual lab results, although in most cases the results themselves are not billable and won’t appear in the claims data. However, billing data is different from traditional requirements and can be used to reach the same endpoint via different routes. For example, it is usually possible to infer the presence or absence of a condition, or its severity, based on downstream claim encounters after the lab was ordered, performed, and read. Medical Data provides the subsequent visits with condition-specific diagnosis codes, while Prescription Data can be used to show subsequent treatments.
How does Medical Data help carriers reduce the time and money spent on APSs?
- Medical Data captures encounters that may not be evidenced in other instant data streams. The breadth of encounters with multiple providers helps to provide a fuller picture of the applicant’s health history, filling in gaps and adding detail to clues that might otherwise have triggered an APS order.
- When an underwriter does need an APS, the use of Medical Data helps carriers ensure that they’re ordering from the most relevant provider and gives underwriters clear guidance about what they’re looking for. This results in:
- Fewer APS orders
- When APSs are needed, orders go to the correct providers who are treating the condition of concern
- Underwriting touch times are reduced, as is time spent waiting on APS reorders
Does the practice of “upcoding” by providers create an unrealistic risk picture, or encourage unnecessary APS orders?
- Although upcoding is a legitimate concern for payers, its impact on mortality risk assessment is mitigated in several ways.
- Most upcoding involves billing for more time, or billing for more expensive procedures, e.g., billing for an MRI while actually using a less-expensive X-ray. Such practices, while fraudulent, are unlikely to influence the mortality outcomes that are most important to underwriters.
- There is an established procedure for applicants to use in order to have erroneous codes removed from their application. If upcoding was having a significant impact on underwriting, we would expect applicants to request such corrections. Our very low FCRA revision rate—currently about 1:2,500 and trending even lower—suggests that upcoding does not result in a significant number of unwarranted conditions appearing in applicant data.
How does the broad spectrum of Medical Data, potentially gathered from many providers, differ from an APS?
- An APS can provide in-depth detail from a single provider who may be a specialist treating a specific condition of concern. Medical Data gathers data from more (and more diverse) providers. For more details related to the breadth of data gathered by Medical Data, please refer to the “What types of data are gathered for Medica Data” question above.
- As a result, Medical Data gives a broader picture of applicant health that, interpreted by the Irix Rules Engine, usually gives an underwriter enough insight to make a decision. Of course, there are still times when an APS may be needed, although Medical Data helps to keep those times to the minimum and ensure that the cost and delay associated with an APS order is well spent.
What can we do to maximize our ROI and minimize our APS orders when using Medical Data?
- Training is the key to quickly getting the most out of Medical Data. Take advantage of initial training and schedule a regroup 60-90 days after starting so that our clinical and actuarial experts can review specific cases and concerns.
- Take advantage of our extensive experience and clinical expertise when calibrating the Irix Rules Engine for your use. For example, make atypical chest pain all green and rely on other rules to assess mortality risk. This helps prevent unnecessary APS orders for conditions that are probably benign but may be concerning for someone not familiar with Medical Data.
- Using Irix Risk Score is another great way to get a “second opinion” about an applicant’s overall mortality risk and can help determine when an APS is likely to be determinative.
When Prescription Data and Medical Data are table stakes tools, APS orders drop significantly.
Medical Data is increasingly fundamental to underwriting efficiency; in fact, it’s a table-stakes requirement alongside Prescription Data for most risk decision-makers. It’s not uncommon for first-time users to see so much more condition insight that they feel compelled to turn to an APS for verification or additional information. Once they’re acclimated to (or proactively trained to embrace) the reality that Medical Data (particularly in combination with Prescription Data) is sufficient to confidently make mortality risk decisions on a large majority of the applicant population, carriers see a net drop in APS orders.
In cases where the additional cost and delay associated with an APS is still warranted, Medical Data makes it easy to target the provider most likely to return a useful APS. Milliman IntelliScript is always ready to help clients adapt underwriting procedures and guidelines to maximize the return on investment from the use of our tools.